 Intra-Cytoplasmic Sperm Injection (ICSI)is recommended for male infertility and it can be applied as part of natural-cycle, minimal-stimulation or full In-Vitro Fertilisation (IVF).
Intra-Cytoplasmic Sperm Injection (ICSI)is recommended for male infertility and it can be applied as part of natural-cycle, minimal-stimulation or full In-Vitro Fertilisation (IVF).
In ICSI, a single sperm is selected and inserted into an egg that has been obtained through IVF treatment. Although ICSI has been routinely used for almost 20 years, it is still considered a major development for the treatment of male infertility. It has been the solution for cases of very low-count, poor-quality and / or difficult to retrieve sperm.
With the use of fine micromanipulator equipment under microscopy, a sperm can be manually injected into an egg, triggering its fertilisation. ICSI is feasible because a sperm is 100 times smaller than an egg.
After fertilisation has occurred, 2-3 days or 5 days later(blastocyst stage),the best quality embryo(s) are selected and transferred back in the womb, as in IVF without ISCI. The number of embryos transferred entirely depends on your individual circumstances.
The end goal of an IVF with ICSI is to have an ongoing, healthy pregnancy followed by a live birth.
ICSI is the method of choice for male infertility, when the availability, quality and / or quantity of sperm are very limited.
Men with a very low-count (small number of sperm in the semen), defected-motility (limited movement) and / or abnormal-morphology (misshaped) sperm are good candidates for ICSI. In these cases, the good quality sperm from their samples, which exist but in a low percentage, are extracted and used for the injection.
This method is also recommended to couples that have a history of previous unsuccessful attempts with IVF.
ICSI may also be the method of choice, if the sperm comes from a frozen sample and its quality / survival after thawing is not as optimum for usage with IVF.
ICSI can also benefit men that have undergone a vasectomy or have azoospermia (lack of sperm in the semen). In these cases, the sperm is collected surgically form the sperm producing and storing tissues in the testicles or the epididymis (a tube structure inside the scrotum where sperm are stored and matured).
Our andrology specialist doctors can give you a full consultation and explain all aspects and risks involved for such procedures, based your individual circumstances. The options may include minor surgery for TEsticular Sperm Extraction (TESE) or Percutaneous Epididymal Sperm Extraction (PESE). Alternatively, microsurgery using a fine needle for the aspiration of sperm from where it is stored in the testes(TEsticular Sperm Aspiration (TESA))or epididymis (Percutaneous Epididymal Testicular Aspiration (PESA))can be employed.
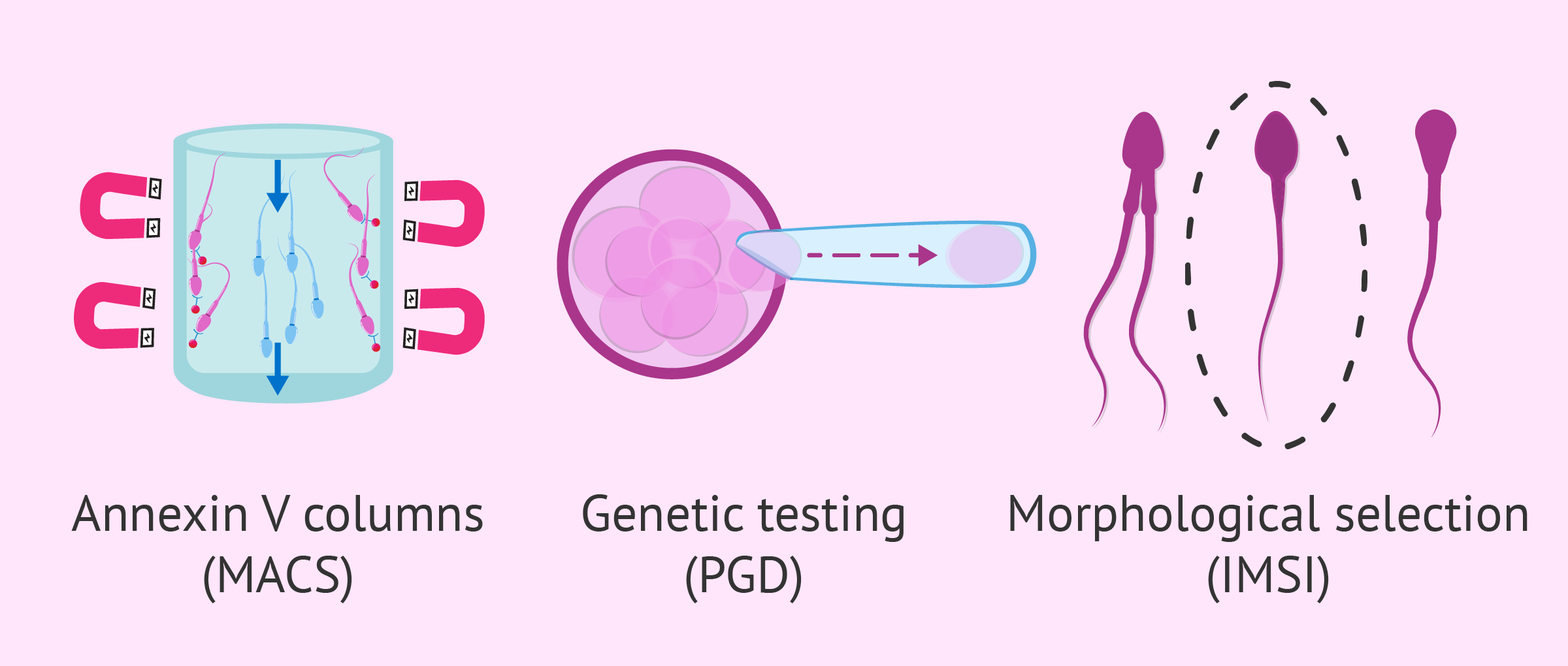
In AAFC, we highly recommend chromosomal testing of embryos obtained by ICSI after a sperm recovery procedure. Hereditary anomalies can be detected through Preimplantation Genetic Diagnosis (PGD) and /or Preimplanation Genetic Screening (PGS).
ICSI requires the sperm and matured egg collection on the same day. For the extra eggs required, an IVF treatment (ovarian stimulation) must be scheduled in advance. The sperm can be sourced on the day of egg collection, through: (a) fresh sperm collection; (b) thawing of a frozen sample; or(c) minor surgery (TESE, PESE) or microsurgery(TESA, PESA). If the procedure of retrieving sperm is estimated to be difficult or time-consuming for it to happen on the same day as egg collection, then it will be carried out before the IVF cycle begins, and the sample will be stored by freezing until needed.
The embryologist, who will assess the sperm before ICSI, examines its morphology (shape) under a microsope and performs a series of diagnostic tests. The best sperm are selected and placed in a dish, until the mature eggs become also available.
Our medical embryologist, next, uses a sharp and hollow needle to pick up a single sperm. A single mature egg is immobilised through the use of a micro manipulation device. The sharp needle carrying the sperm is then driven to pierce the egg, and the sperm is released into its core. The needle is carefully retracted and the inseminated egg is placed in a dish and back in the incubator. The procedure is carefully repeated for all the available eggs.
The rest of the steps: fertilization, embryo transfer, first pregnancy test and ultrasound scan are performed exactly the same as in IVF. PGD or PGS testing for any chromosomal abnormalities can be performed before embryo transfer.
ICSI has been used in nearly half of all the IVFs performed and the two techniques share a very similar success rate.
About 70-85% of the eggs injected with sperm in ICSI become fertilised. However, the overall outcome of ICSI depends on your individual circumstances. Chromosomal integrity of the sperm used and maternal age are the two main factors responsible for a negative outcome. Normally, younger women exhibit a high percentage of success with ICSI, but that declines dramatically with women over 45.
If ICSI was not a success, AAFC will offer you support. Our specialist doctors will provide you with a comprehensive consultation for all other available / applicable options, and with explanations, where possible, for the reasons behind a negative outcome.